Rectal prolapse (rectal prolapse) is a downward displacement of the rectum with its exit (evering) through the anus.
The incidence of rectal prolapse is 9-10% of all colon .
Content
Degree of disease development
Depending on the degree of development of the disease, rectal prolapse is divided into:
- prolapse of the mucous membrane;
- prolapse of the anus;
- internal intussusception of the rectum;
- rectal prolapse;
- prolapse of the invaginated rectum.
Causes of rectal prolapse
There are two main reasons for the development of the disease:
- increased intra-abdominal pressure;
- weakening of the supporting ligamentous apparatus of the rectum.
Increased intra-abdominal pressure can occur when:
- childbirth;
- constipation;
- lifting weights.
Weakening of the supporting apparatus of the pelvis and rectum can be caused by both anatomical:
- long mesentery of the sigmoid colon;
- small concavity of the sacrum,
and physiological reasons:
- exhaustion;
- disruption of intestinal innervation,
- previous intestinal diseases (colitis, dysentery ).
 Prolapse of all layers of the rectum is possible if at least one of the following risk factors is present:
Prolapse of all layers of the rectum is possible if at least one of the following risk factors is present:
- weakening of the pelvic floor muscles;
- weakening of the abdominal muscles;
- weakness of the internal and external anal sphincters;
- severe general exhaustion;
- anatomical features of the structure of the mesentery.
With such risk factors, any tension in the press is enough for intestinal prolapse to occur.
According to V.G. Vorobyov, the impetus for the development of this disease was:
- heavy physical work - in 37% of patients;
- persistent constipation - 40%;
- trauma - 13%;
- childbirth - in 7% of women;
- diarrhea and significant decrease in body weight - in 3%.
Repeated rectal prolapse can occur when sneezing, coughing, or defecation.
Symptoms
The symptoms of this disease differ from other diseases of the rectum. If the disease develops gradually, the pain may be absent or not as acute as with hemorrhoids or anal fissure.
The gradual development of rectal prolapse is more common. The first time rectal prolapse occurs when straining during defecation and is easily eliminated on its own. Gradually, after each bowel movement, it becomes necessary to straighten the rectum by hand. If no measures are taken, rectal prolapse occurs when coughing, standing in an upright position, or sneezing.
If it develops suddenly (for example, when lifting a heavy object), the pain can be so unexpected and severe that collapse is possible.
Typically, rectal prolapse is accompanied by symptoms such as:
- sensation of a foreign body in the anus,
- pain in the lower abdomen,
- pain in the anus,
- discharge of large amounts of mucus during bowel movements,
- feeling of wetness in the anus,
- false urge to defecate,
- incontinence of gases and feces,
- itching,
- bleeding due to damage to the intestinal mucosa,
- may sometimes be accompanied by urinary incontinence.
Diagnostics
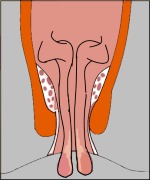
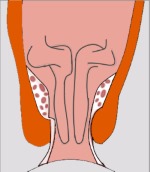
The diagnosis is made during a proctological examination . The patient is asked to push in a squatting position.
Upon examination, the prolapsed section of the rectum has the shape of a cone, cylinder or ball of a bright red or bluish hue with a slit-like or star-shaped opening in the center. There is moderate swelling of the mucous membrane and slight bleeding on contact.
 Much less common is internal rectal prolapse, that is, the descent of the overlying parts of the rectum into the underlying ones. As a rule, this type of intussusception is not detected by digital examination.
Much less common is internal rectal prolapse, that is, the descent of the overlying parts of the rectum into the underlying ones. As a rule, this type of intussusception is not detected by digital examination.
Carrying out a digital rectal examination allows you to assess the tone of the sphincter, distinguish rectal prolapse from hemorrhoids, low-lying anal polyps and prolapse through the anus.
Pathology can be detected by irrigoscopy or proctography (fluoroscopy) with straining.
X-rays of the rectum at rest and with straining show changes characteristic of hidden rectal prolapse. These include a mushroom-shaped deformity of the rectum or a spherical subcutaneous prolapse of the anterior wall of the rectum through a defect in the perineal muscles.
It is also useful to conduct functional studies - scintidedefecography and electrophysiological studies of the motor function of the colon.
In 71% of patients with internal rectal prolapse, a rectal ulcer is detected.
Sigmoidoscopy allows you to determine the presence of an ulcer on the wall of the rectum and intussusception.
Colonoscopy can rule out diseases such as diverticulosis, tumors and other diseases.
When performing anorectal manometry , the function of the muscles surrounding the rectum and their participation in the process of defecation are assessed.
Women with rectal prolapse should consult a gynecologist.
Treatment
 If the rectum prolapses, it must be immediately corrected.
If the rectum prolapses, it must be immediately corrected.
If this is not done, the intestine swells and then it is difficult to insert it. The swelling grows quickly and the blood supply to the tissues is disrupted, which can lead to necrosis of the area of the prolapsed rectum.
The most dangerous is the simultaneous displacement of the loops of the small intestine into the peritoneal pouch - in this case, intestinal obstruction may develop. In adults, intestinal reduction is performed in the knee-elbow position or on the left side. Reduction of the prolapsed intestine leads to the restoration of blood flow and the normal appearance of the mucous membrane.
Minimally invasive treatment methods include the introduction of sclerosing drugs and electrical stimulation of the pelvic floor and sphincter muscles. However, these methods are advisable in the initial stages of the disease.
In advanced forms, surgical treatment is necessary.
In case of prolapse of the mucous membrane of the anal canal, a relatively simple method of excision of the prolapsed area is used. As a rule, this operation is combined with ligation and excision of internal hemorrhoids.
Prolapse of all layers of the rectum also requires surgical treatment, but in this case it is much more complicated.
There are a number of surgical techniques:
- narrowing the anal opening using a silver wire,
- fixation of the rectum from the perineal side,
- intra-abdominal fixation,
- various types of sphincteroplasty,
- implantation of a magnetic obturator device.
Since there are usually several causes of rectal prolapse at the same time (relaxation of the anal sphincter, weakening of the muscles that lift the anus, in combination with impaired fixation of the rectum in the pelvis), various methods of combined surgical treatment are often used.
All types of surgical operations are divided into three groups:
- perineal,
- cavitary,
- laparoscopy.
The choice of surgical technique is dictated by the age, physical condition of the patient, causes and degree of rectal prolapse.
 The indication for surgical treatment of rectal prolapse is the absence of positive results from conservative measures carried out within 2 months.
The indication for surgical treatment of rectal prolapse is the absence of positive results from conservative measures carried out within 2 months.
If surgical treatment is not possible, the use of bandages is recommended.
Prevention
The main thing in preventing the disease is taking care of good bowel function. It is important to avoid constipation and hard stool.
You can read about the treatment and prevention of constipation in the article “ Constipation ”.
Rectal prolapse in children
In children, this disease occurs in the first years of life. Prolapse of the mucous membrane of the anal canal occurs as a result of prolonged diarrhea or persistent constipation. The most common cause is hemorrhoids. But the cause can also be the genetic disease cystic fibrosis.
If a child's rectum has prolapsed, it must be realigned, following these rules.
- Raise your legs and spread them apart.
- Generously lubricate the prolapsed intestine with Vaseline.
- Using your hand, carefully move it into the pelvic area, screwing the central part into the intestinal lumen.
- The part of the intestine located closer to the anus, as a rule, is reduced on its own.
In children at an early age, this disease can be eliminated without surgery. If you take certain measures, the disease may not recur.
- Do not strain during bowel movements.
- Do not put your child on the potty for some time.
- Don't let him scream.
- Stop diarrhea with fixatives.
- For constipation, give enemas.